")
")
")
Download the full article "Total Motor Score (TMS) v.3 --- A Proposed Kinematic Measure of Speech Motor Control and Complexity".
Total Motor Score (TMS) v.3:
A Proposed Kinematic Measure of Speech Motor Control and Complexity
My Framework: Quantifying Motor Load for Functional Progress
My approach is built on the reality that we must start with words that matter to the child—words like HOME. I use my TMS (Total Motor Score) to calculate the exact "cost" of that word. For example, if HOME (/hoʊm/) has a calculated TMS of 5.0, that becomes our starting point. We aren't just practicing a word; we are practicing a specific level of motoric demand.
1. Establishing Stability (Blocked Practice)
We begin with the functional word the child needs. If the target is HOME, we use Blocked Practice, repeating that specific motor plan.
- The Science: Research in Dynamic Temporal and Tactile Cuing (DTTC) emphasizes that in the acquisition phase, we need high-frequency repetition to "groove" the neural pathway.
- The Goal: We stay here until the child moves from "random success" to consistency. We want the child to find that specific map for HOME every time they try.
2. The Generalization Bridge (Variable Practice)
Once HOME is stable, the real work of overcoming CAS begins. We cannot stop at one word; we must generalize the motor skill. This is where my theory of Motor Equivalence is applied.
- The Strategy: I identify other words that have the same TMS (5.0) and Layer 2 (Basic Shape).
- The Action: We move into Variable Practice, switching between HOME and these other equally-weighted motor plans.
- The Science: This follows the Contextual Interference Effect. By keeping the "weight" (TMS) the same but changing the "targets" (the words), we force the brain to re-plan the movement every time. This is how we move from a memorized word to a generalized ability to speak.
Total Motor Score (TMS) v.3:
A Proposed Kinematic Measure of Speech Motor Control and Complexity
Preface: An Emerging Research Model
The Total Motor Score (TMS) v.3 is a proposed clinical framework designed to assist Speech-Language Pathologists (SLPs), Speech-Language Pathologist Assistants (SLPAs), Communicative Disorders Assistants (CDAs), teachers, and other professionals working directly on speech motor intervention. The framework is intended for use with both pediatric and adult populations presenting with motor speech disorders, including Childhood Apraxia of Speech (CAS), Apraxia of Speech (AOS), and motor planning impairments associated with aphasia.
Unlike traditional phonological metrics such as Percentage of Consonants Correct (PCC), the TMS emphasizes spatiotemporal and kinematic aspects of speech production, including articulatory movement trajectories, sequencing demands, and inter-articulator coordination. The TMS v.3 is presented as an emerging, theoretically informed heuristic to support intervention planning and target sequencing, rather than as a diagnostic or normative assessment tool.
The Two-Layer Framework
The complexity of a target word is analyzed through two distinct layers:
- Layer 1 - The TMS Core Score (Numeric): A calculated value representing the baseline motoric demand.
- Layer 2 - Structural Progression Rules (Qualitative): Guidelines used to organize the order of treatment targets.
I. Introduction: The Clinical Rationale
Current assessment standards provide essential diagnostic information but often fail to capture the dynamic gestural transitions required for fluent speech. In motor speech disorders, breakdowns frequently occur during the movement from one articulatory posture to the next, particularly as sequencing demands increase.
The TMS v.3 addresses this gap by quantifying the motoric complexity of speech targets through four primary variables:
- Mandibular Grading: Control of jaw height across varying degrees of oral openness.
- Lingual–Mandibular Dissociation: The independence of tongue movement from jaw position.
- Trajectory Complexity: Articulatory transitions requiring graded movement (diphthongs, rhotics).
- Syllabic Load: Sequencing demands arising from consonant and vowel transitions within multisyllabic words.
II. The Modeling Formula (TMS v.3)
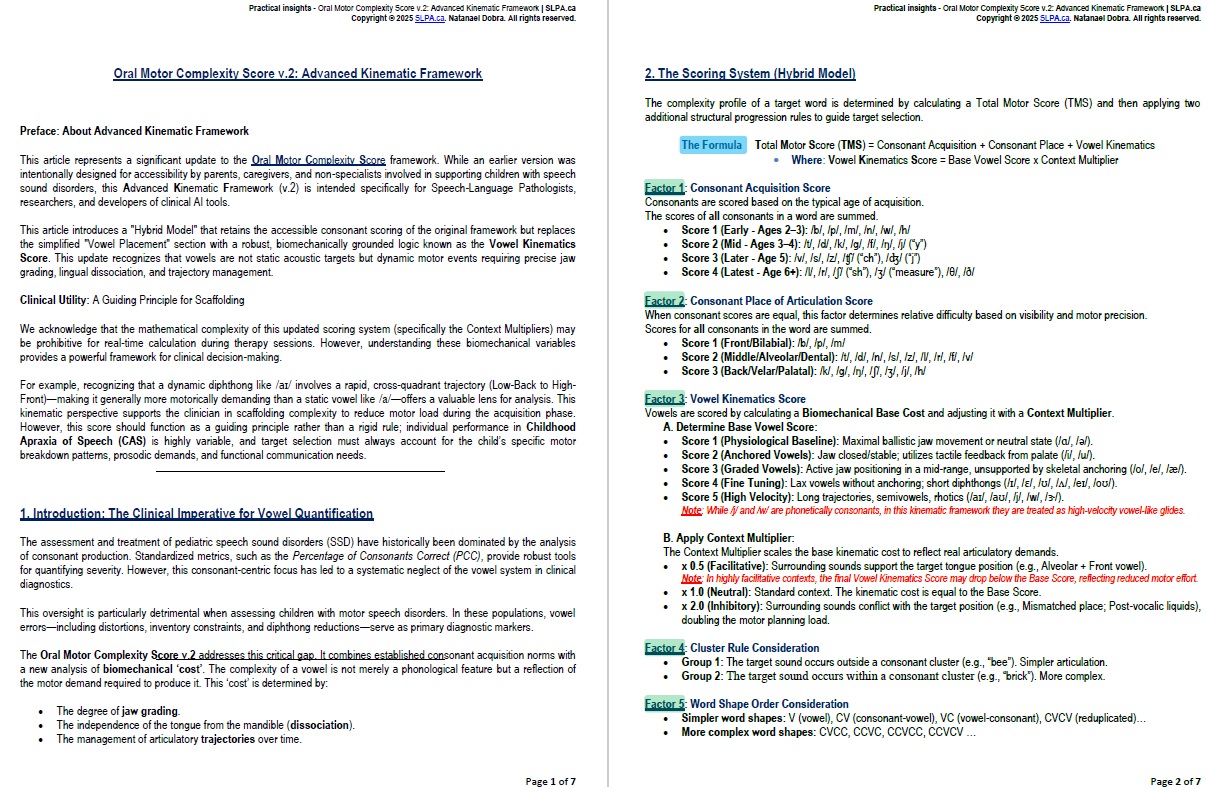
The complexity profile of a target word is determined by calculating a Total Motor Score (TMS) and then applying Structural Progression Rules to guide target selection.
Total Motor Score (TMS) = CAS + CPS + VKS + ST
Where:
- CAS (Consonant Acquisition Score) = Sum of developmental difficulty scores for all consonants
- CPS (Consonant Place of Articulation Score) = Sum of scores based on articulatory placement
- VKS (Vowel Kinematics Score) = Sum of (Base Vowel Score × Context Multiplier) for all vowels
- ST (Sequencing Tax) = Cost associated with syllable number and sequencing load.
III. Layer 1: Numeric Factors
Factor 1: Consonant Acquisition Score (CAS)
Consonants are scored based on the typical age of acquisition.
The scores of all consonants in a word are summed.
- Score 1 (Early - Ages 2–3): /b/, /p/, /m/, /n/, /w/, /h/
- Score 2 (Mid - Ages 3–4): /t/, /d/, /k/, /g/, /f/, /ŋ/, /j/ (“y”)
- Score 3 (Later - Age 5): /v/, /s/, /z/, /ʧ/ (“ch”), /ʤ/ (“j”)
- Score 4 (Latest - Age 6+): /l/, /r/, /ʃ/ (“sh”), /ʒ/ (“measure”), /θ/, /ð/
Factor 2: Consonant Place of Articulation Score (CPS)
Determines relative difficulty based on visibility and motor precision.
Scores for all consonants in the word are summed.
- Score 1 (Front/Bilabial): /b/, /p/, /m/, /w/
- Score 2 (Middle/Alveolar/Dental): /t/, /d/, /n/, /s/, /z/, /l/, /r/, /f/, /v/, /θ/, /ð/
- Score 3 (Back/Velar/Palatal): /k/, /g/, /ŋ/, /ʃ/, /ʒ/, /j/, /h/, /ʧ/, /ʤ/
Factor 3: Vowel Kinematics Score (VKS)
Vowels are scored by calculating a Biomechanical Base Cost and adjusting it with a Context Multiplier.
A. Determine Biomechanical Base Vowel Score:
- Score 1 (Physiological Baseline): Maximal ballistic jaw movement or neutral state (/ɑ/, /ə/).
- Score 2 (Anchored Vowels): Jaw closed/stable; utilizes tactile feedback from palate (/i/, /u/).
- Score 3 (Graded Vowels): Active jaw positioning in a mid-range, unsupported by skeletal anchoring (/o/, /e/, /æ/, /ɔ/).
- Score 4 (Fine Tuning): Lax vowels without anchoring; short diphthongs (/ɪ/, /ɛ/, /ʊ/, /ʌ/, /eɪ/, /oʊ/).
- Score 5 (High Velocity): Long trajectories, semivowels, rhotics (/aɪ/, /aʊ/, /j/, /w/, /ɝ/).
Note: While /j/ and /w/ are phonetically consonants, in this kinematic framework they are treated as high-velocity vowel-like glides.
B. Apply Context Multiplier:
The Context Multiplier scales the Base Vowel Score to reflect real-world articulatory demands.
This multiplier is determined by Co-Articulation Compatibility—the specific biomechanical relationship between the target consonant and the adjacent vowel.
- x 0.5 (Facilitative): Surrounding sounds support the target tongue position (e.g., Alveolar + Front vowel).
Note: In highly facilitative contexts, the final Vowel Kinematics Score may drop below the Base Score, reflecting reduced motor effort.
- x 1.0 (Neutral): Standard context. The kinematic cost is equal to the Base Score.
- x 2.0 (Inhibitory): Surrounding sounds conflict with the target position (e.g., Mismatched place; Post-vocalic liquids), doubling the motor planning load.
*For a complete list of compatibility rules by sound class, see Annex A: Master Library of Co-Articulation Compatibility.
Note on Stacking: In complex phonetic environments where multiple co-articulatory constraints apply, multipliers are cumulative (stacked). For example, a lax vowel (Base 4) followed by a post-vocalic liquid (x2.0) in an inhibitory jaw context (x2.0) would result in a total VKS of 16.0 (4×2×2).
Remember: VKS = (Base Score × Multiplier). If a word has multiple vowels, you sum them together.
The Base Score is the "starting cost" of the vowel in a vacuum, and the Multiplier is how the surrounding consonants change that cost.
VKS Examples
1. Bee (/bi/) - Vowel: /i/
- Base Score: 2 (Anchored Vowel - jaw stable, tactile feedback from palate).
- Context: Bilabial (/b/) + Front Vowel (/i/).
Multiplier: x 1.0 (Neutral). While /b/ doesn't conflict with /i/, Annex A (Section 1.B) notes it doesn't mechanically "assist" the jaw spread/height for /i/ the way it does for central vowels.
VKS = 2×1.0 = 2
2. Brick (/brɪk/) - Vowel: /ɪ/
- Base Score: 4 (Fine Tuning - lax vowel without anchoring).
- Context: Rhotic Liquid (/r/) + Lax Vowel (/ɪ/).
Multiplier: x 2.0 (Inhibitory). Per Annex A (Section 4.B), rhotics create 'Liquid Conflict' and double the planning load (×2.0 inhibitory) for the following vowel. While Annex A emphasizes this for round and low vowels, in CAS the instability of a pre-vocalic /r/ often increases the load for lax vowels like /ɪ/ as well.
VKS = 4×2.0 = 8
3. Mummy (/mʌ.mi/) - This word has two vowels, so we calculate each and add them.
Vowel 1 (/ʌ/):
- Base Score: 4 (Fine Tuning/Lax). For lax vowels like /ʌ/, the tongue does not contact the teeth or palate, providing no external tactile “landing pad.” As a result, production relies more on proprioceptive feedback to stabilize a central tongue posture, which increases motor-planning demands compared to vowels with clear contact points.
- Context: Bilabial /m/.
Multiplier: ×0.5 (Facilitative). Annex A (Section 1.B) notes that bilabials facilitate central vowels due to a shared relaxed jaw posture. The bilabial /m/ and the vowel /ʌ/ are motorically compatible, allowing efficient transitions between consonant and vowel with minimal jaw reconfiguration.
VKS1 = 4×0.5 = 2.
Vowel 2 (/i/):
- Base Score: 2 (Anchored). The vowel /i/ is considered an anchored vowel due to lingual–palatal contact. During /i/, the lateral edges of the tongue contact the upper molars and palate, providing strong tactile feedback that supports tongue placement and reduces motor-planning demands compared to non-anchored vowels such as /ʌ/
- Context: Bilabial /m/.
Multiplier: x 1.0 (Neutral). Although the jaw remains high, facilitating /m/, production of /i/ requires increased lingual tension and elevation. This tongue configuration neither facilitates nor interferes with bilabial closure, so overall motor effort remains neutral.
VKS2 = 2×1.0 = 2.
VKS = VKS1 + VKS2 = 2+2=4
4. Banana (/bə.næ.nə/) - This word has three vowels.
Vowel 1 (/ə/):
- Base Score: 1 (Baseline). The schwa /ə/ is the neutral state of the vocal tract with minimal muscle activation.
- Context: Bilabial /b/
Multiplier: x 0.5 (Facilitative). Per Annex A (Section 1.B), the relaxed jaw of the neutral vowel helps the lips close for the /b/. Because the jaw & lips work together so efficiently here, the motor effort is "discounted" by half.
VKS1 = 1×0.5 = 0.5.
Vowel 2 (/æ/):
- Base Score: 3 (Graded). The vowel /æ/ requires the jaw to be held in a precise mid-low position without touching any part of the mouth for support. This requires active muscular control of the jaw height.
- Context: Alveolar /n/.
Multiplier: x 1.0 (Neutral). While the tongue tip is forward for /n/, the wide jaw drop required for /æ/ does not provide a specific biomechanical "assist" to the alveolar ridge contact. They do not conflict, but they aren't "friends" like the first syllable, so the cost remains standard.
VKS2 = 3×1.0 = 3
Vowel 3 (/ə/):
- Base Score: 1 (Physiological Baseline). The neutral schwa.
- Context: Alveolar /n/.
Multiplier: x 1.0 (Neutral). Unlike the lip closure in the first syllable, the tongue-tip contact for /n/ is naturally independent of the neutral jaw state of /ə/. It is a standard, efficient transition without a specific facilitating "discount."
VKS3 = 1x1.0 = 1
VKS = VKS1 + VKS2 + VKS3 = 0.5+3+1 = 4.5
Factor 4: Sequencing Tax (ST)
The Sequencing Tax (ST) measures the incremental motoric and cognitive load incurred during the production of multisyllabic words. Unlike static measures, the ST focuses on the articulatory transition cost—the degree of change required to shift from one motor program (Sn−1) to the next (Sn).
The tax is calculated cumulatively for each syllable beginning with the second (n≥2).
· Factor 4.1: The Incremental Cost Rule
Each subsequent syllable is compared to the syllable immediately preceding it, and motoric cost is determined by the degree of segmental and structural overlap between adjacent syllables.
- Total Reduplication (Exact Copy): +0.0
The onset and nucleus (C and V) are identical, and the syllable shape is unchanged (CV–CV), as in mama, papa, or bye–bye. The existing motor program is re-executed, requiring minimal additional planning.
- Partial Reduplication / Segmental Alternation: +0.5
Either the consonant (C) or the vowel (V) changes, but not both, while the syllable shape remains constant (CV–CV), as in mami or midi. The syllabic motor frame or segmental target is partially reused, requiring modification of a single articulatory parameter.
- Varied Syllable (No Shared Segments): +1.0
Both the consonant and vowel differ from the preceding syllable, as in banana, piano, or tomato. A new speech motor program must be planned and assembled, placing maximal demand on the sequencing buffer.
· Factor 4.2: Structural Shift Penalty
- Any change in the syllable template (e.g., CV → CVC, or CV → VC) incurs an additional cost of +0.5. This reflects the extra motoric effort required to recalibrate temporal coordination and gestural timing when syllable shape changes. The cost is additive, stacking on top of any segmental differences between syllables.
- When a diphthong-final syllable (/aɪ/, /aʊ/, /ɔɪ/, /eɪ/, /oʊ/) transitions to a vowel-initial or VC syllable containing /ɹ/, /ɝ/, or /l/, add +0.75 to ST. This accounts for heightened planning load in rhotic/liquid re-alignment after high-velocity nuclei.
Summary
Sequencing Tax for a word is the sum of the transition costs between all adjacent syllables:
![]()
ST Examples
1. Mummy (/mʌ.mi/)
The word mummy has two syllables: (S1) - /mʌ/ followed by (S2) - /mi/.
- Syllable 1 (S1): /mʌ/ - (This is the baseline, no tax yet).
- Syllable 2 (S2): /mi/
Step A: Compare Segments - The consonant remains the same (/m/ → /m/)
- S1 S2 - The vowel changes (/ʌ/ → /i/).
- Only one segment changed → Segmental cost = +0.5
Step B: Compare Shape - Shape: CV → CV (No change)
- S1 S2 - The shape has not changed → Shape cost = +0.0
Total Sequencing Tax (ST): 0.5 (segmental) + 0.0 (shape) = 0.5 ST
The syllable shape (CV) is unchanged. According to the Incremental Cost Rule, this counts as Partial Reduplication / Segmental Alternation, with a tax of +0.5. Therefore, the total Sequencing Tax for mummy is 0.5.
2. Table (/teɪ.bəl/)
The word table has two syllables: (S1) - /teɪ/ followed by (S2) - /bəl/.
- Syllable 1 (S1): /teɪ/ - (This is the baseline, no tax yet).
- Syllable 2 (S2): /bəl/
Step A: Compare Segments - Consonant: /t/ → /b/ (change)
- S1 S2 - Vowel: /eɪ/ → /ə/ (change)
- Both consonant and vowel changed → Segmental cost = +1.0
Step B: Compare Shape - Syllable shape: CV → CVC (change)
- S1 S2 - The shape changed → Shape cost = +0.5
Total Sequencing Tax (ST): 1.0 (segmental) + 0.5 (shape) = 1.5 ST
Table consists of two syllables: /teɪ/ and /bəl/. From the first to the second syllable, both consonant and vowel change (/t/ → /b/, /eɪ/ → /ə/), and the syllable shape shifts from CV to CVC. The change in segments corresponds to a Varied Syllable, contributing +1.0 to the tax, while the structural shift adds an additional +0.5. Summing these, the Sequencing Tax for table is 1.5.
3. Banana (/bə.næ.nə/)
The word banana has three syllables: (S1) - /bə/ followed by (S2) - /næ/ followed by (S3) - /nə/.
- Syllable 1 (S1): /bə/ - (This is the baseline, no tax yet).
- Syllable 2 (S2): /næ/
- Syllable 3 (S3): /nə/
Step A: Compare Segments - Consonant: /b/ → /n/ (change)
- S1 S2 - owel: /ə/ → /æ/ (change)
- Both consonant and vowel changed → Segmental cost = +1.0
- S2 S3 - The consonant remains the same (/n/ → /n/)
- Vowel: /æ/ → /ə/ (change)
- Only one segment changed →
Step B: Compare Shape - Shape: CV → CV → CV (No change)
- The shape has not changed → Shape cost = +0.0
Total Sequencing Tax (ST): 1.0 (segmental) + 0.5 (segmental) + 0.0 (shape) = 1.5 ST
The word banana has three syllables: /bə/, /næ/, and /nə/. The first transition, from /bə/ to /næ/, involves a change in both consonant and vowel, with the syllable shape unchanged. This counts as a Varied Syllable, giving +1.0. The second transition, from /næ/ to /nə/, keeps the consonant the same (/n/) while changing the vowel (/æ/ → /ə/), fitting Partial Reduplication / Segmental Alternation with a cost of +0.5. Adding these together, the total Sequencing Tax for banana is 1.5.
Clinical Note:
In this framework, absolute numbers are less important than relative complexity.
Note how a facilitative context can reduce a vowel's contribution, while inhibitory contexts can drastically spike the difficulty.
IV. Layer 2: Structural Progression Rules
These qualitative rules do not modify the numeric TMS but organize the hierarchy of treatment.
Rule A: Consonant Cluster Consideration
- Group 1: Words containing consonants, none of which form a cluster (e.g., bee, cat).
- Group 2: Words containing consonant clusters (e.g., brick, stamp).
Because clusters require additional articulatory coordination, they should be introduced only after accuracy with words containing single, non-clustered consonants is well established.
Rule B: Word Shape Order
- Basic Shapes:
Targets should start with non-clustered syllables, including vowels (V) (e.g., a, o), consonant–vowel (CV) (e.g., ma, ta), vowel–consonant (VC) (e.g., up, an), and CVC (e.g., cat, dog). Early multisyllabic productions often involve reduplication, which can be total (e.g., mama), partial (e.g., mami), or varied (e.g., piano). These shapes have minimal motoric demand and provide the foundation for introducing more complex words.
- Complex Shapes:
Once basic shapes are mastered, words containing consonant clusters are introduced, organized by increasing complexity: CCV (e.g., play, tree), CCVC (e.g., stop, brick), CVCC (e.g., desk, milk), and CCVCC (e.g., plant, stomp). Multisyllabic words may combine these clusters across syllables (e.g., stapler, splendid), requiring sequencing and coordination of multiple motor programs. These complex shapes are addressed only after stable production of non-clustered syllables, reflecting the natural progression of motor planning in speech development.
V. Word Examples (Applied v.3 Scoring) - Total Motor Score (TMS)
- Bee (/bi/) — Shape: CV (1 Syllable)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /b/ (1) + CPS: /b/ (1) = 2
- VKS: /i/ (Base 2 × Neut. 1.0) = 2
- ST: Single syllable = 0
TOTAL MOTOR SCORE (TMS): 4
Layer 2 – Structural Progression Rules
- Cluster: Group 1
- Shape: CV — Simpler word shapes
Rationale: As per Annex A (Section 1.B), bilabials are neutral with front vowels. While the spread lips of /i/ do not conflict with /b/, they do not mechanically "assist" jaw closure in the same way central vowels do.
- Bin (/bɪn/) — Shape: CVC (1 Syllable)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /b/ (1) + /n/ (1) + CPS: /b/ (1) + /n/ (2) = 5
- VKS: /ɪ/ (Base 4 × Facil. 0.5) = 2
- ST: Single syllable = 0
TOTAL MOTOR SCORE (TMS): 7
Layer 2 – Structural Progression Rules
- Cluster: Group 1
- Shape: CVC — Simpler word shapes
Rationale: Despite /ɪ/ being a difficult lax "floating" vowel, the alveolar coda /n/ facilitates it. The tongue tip anchors on the ridge, providing stability and reducing motor planning effort (Annex 2.B).
- Bulb (/bʌlb/) — Shape: CVCC (1 Syllable)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /b/ (1) + /l/ (4) + /b/ (1) + CPS: /b/ (1) + /l/ (2) + /b/ (1) = 10
- VKS: /ʌ/ (Base 4 × Inhib. 2.0) = 8
- ST: Single syllable = 0
Total Motor Score (TMS): 18
Layer 2 – Structural Progression Rules
- Cluster: Group 2
- Shape: CVCC — Complex word shapes
Rationale: Score spikes due to "Liquid Conflict." The post-vocalic /l/ creates a high motor planning load, doubling the vowel kinematics cost.
- Brick (/brɪk/) — Shape: CCVC (1 Syllable) Layer 1 – The TMS Core Score (Numeric):
- CAS: /b/ (1) + /r/ (4) + /k/ (2) + CPS: /b/ (1) + /r/ (2) + /k/ (3) = 13
- VKS: /ɪ/ (Base 4 × Inhib. 2.0) = 8
- ST: Single syllable = 0
Total Motor Score (TMS): 21
Layer 2 – Structural Progression Rules
- Cluster: Group 2
- Shape: CCVC — Complex word shapes
Rationale: Highest single-syllable complexity. Combines late-acquired consonants, a cluster, and an inhibitory liquid context that doubles the vowel cost.
- Mummy (/mʌ.mi/) — Shape: CV.CV (2 Syllables)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /m/ (1) + /m/ (1) + CPS: /m/ (1) + /m/ (1) = 4
- VKS: /ʌ/ (4 × 0.5 Facil.) + /i/ (2 × 1.0 Neut.) = 4
- ST: Partial Reduplication (C same, V changes) = 0.5
Total Motor Score (TMS): 8.5
Layer 2 – Structural Progression Rules
- Cluster: Group 1
- Shape: CV.CV — Simpler word shapes
Rationale: Bilabial /m/ facilitates central /ʌ/ because a relaxed jaw aids closure. Motor load is reduced via partial reduplication, as the brain reuses the existing motor program for /m/.
- Table (/teɪ.bəl/) — Shape: CV.CVC (2 Syllables)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /t/ (2) + /b/ (1) + /l/ (4) + CPS: /t/ (2) + /b/ (1) + /l/ (2) = 12
- VKS: /eɪ/ (4 × 1.0) + /ə/ (1 × 2.0 Inhib. Liquid) = 6
- ST: Varied (1.0) + Structural Shift (0.5) = 1.5
Total Motor Score (TMS): 19.5
Layer 2 – Structural Progression Rules
- Cluster: Group 1*
- Shape: CV.CVC — Complex word shapes
Rationale: Complexity is driven by the post-vocalic /l/ in the second syllable, which doubles the kinematic cost of the schwa. The structural shift (CV to CVC) adds extra motoric effort to recalibrate timing.
- Banana (/bə.næ.nə/) — Shape: CV.CV.CV (3 Syllables)
Layer 1 – The TMS Core Score (Numeric):
- CAS: /b/ (1) + /n/ (1) + /n/ (1) + CPS: /b/ (1) + /n/ (2) + /n/ (2) = 8
- VKS: /ə/ (1 × 0.5 Facil.) + /æ/ (3 × 1.0 Neut.) + /ə/ (1 × 1.0 Neut.) = 4.5
- ST: Varied (1.0) + Partial (0.5) + Structural Shift Penalty (0.5) = 2.0
Total Motor Score (TMS): 14.5
Layer 2 – Structural Progression Rules
- Cluster: Group 1
- Shape: CV.CV.CV — Simpler word shapes
Rationale: While individual sounds are developmentally early, the 3-syllable load drives complexity. The transition from a Graded Vowel (/æ/) to a Baseline Vowel (/ə/) triggers a structural shift penalty.
.
VI. Scientific Framework
This section explains the science behind the Total Motor Score (TMS) v.3. It describes how we measure the physical effort of speech by looking at how the mouth moves. This framework updates traditional scoring to include Vowel Kinematics (the effort of the tongue and jaw) and the Sequencing Tax (the effort of switching between syllables).
6.1 Anatomical Foundations: The "Moving Target"
To accurately score a word, we must understand that a child’s mouth is physically different from an adult’s:
- Vocal Tract Length (VTL):
A baby’s vocal tract is very short (6–8 cm). As the child grows to an adult (15–18 cm), the "tube" of the throat changes.
- The Moving Target Hypothesis:
Because the child’s mouth is constantly growing, the brain must constantly "re-learn" how to hit the right spots to make sounds.
- Laryngeal Descent:
In infants, the voice box (larynx) is very high. As it moves down during childhood, it creates the space needed for the tongue to pull back for deep sounds like /ɑ/ (as in "hot").
6.2 Motor Control Variables
We measure complexity by looking at how the different parts of the mouth work together:.
- Mandibular Control (The Jaw):
- Easy (Ballistic) - Endpoint-anchored movements (Low Complexity):
Targets in which jaw positioning occurs near biomechanical end ranges (e.g., /a/ with a relatively open jaw), allowing skeletal limits and consistent proprioceptive feedback to support movement execution.
Reduced need for fine-grained jaw positioning may lower motoric demands during intervention.
- Hard (Graded) jaw movements - (High Complexity):
Sounds where the jaw has to hover in the middle (like /e/ or /o/). This requires the muscles to hold a very steady, precise position..
- Lingual–Mandibular Dissociation (Tongue and Jaw Independence):
Differentiates speech targets based on the degree of independence required between lingual movement and mandibular position.
- Coupled movements: Targets in which lingual posture is largely determined by jaw position, resulting in reduced motoric degrees of freedom (e.g., /a/ with a relatively open jaw and minimal lingual shaping). The tongue just follows the jaw. (Easy).
- Decoupled movements: Targets that require active lingual movement independent of the jaw, increasing coordination demands (e.g., producing /i/ with a relatively lowered or stabilized jaw, necessitating active tongue elevation). The tongue has to move high while the jaw stays low (/i/). This requires the tongue and jaw to work independently. (Hard)
- Velopharyngeal Valving (Airflow/Resonance Control):
Distinguishes between speech targets that require
- Sustained velopharyngeal posture (e.g., “mama”, in which velopharyngeal opening is maintained across the utterance),
- Dynamic velopharyngeal switching (e.g., “ant”, which requires rapid transitions between velopharyngeal closure and opening across adjacent segments).
Targets requiring dynamic switching impose greater motoric complexity due to increased demands on timing precision, movement reversals, and coordination between the velopharyngeal mechanism and oral articulators.
- Trajectories (Distance and Speed):
- Complexity is based on the distance the tongue travels. A sound like /aɪ/ (as in "bye") requires the tongue to travel a long way very fast. If a child says "bak" instead of "bike," they are trying to save energy by not moving their tongue as far.
6.3 Developmental Chronology & Limitations
The scoring follows how children naturally grow: "Corner Vowels" (/i/, /u/, /ɑ/) usually come first, then "floating" vowels, and finally "R-sounds" (Rhotics)
Limitations of the Framework:
While plausible, the specific hierarchy of the Vowel Kinematics Score is currently theoretical. There are no published studies confirming that /e/ is universally "harder" than /ɑ/ for all children with CAS, as individual variability in motor planning is significant. Furthermore, clinical success relies on multifactorial intervention (prosody, intensity, feedback) rather than target selection alone. Future research is required to validate these scoring metrics against kinematic instrumentation, such as ultrasound imaging. Success in therapy depends on many things, like how often the child practices and the feedback they get, not just picking the right words.
VII. Clinical Observations: Balancing Complexity with Functionality
While this framework emphasizes the quantification of motor difficulty, successful intervention requires balancing biomechanical constraints with functional communication goals.
7.1 The Motor–Functional Paradox
Children with CAS struggle to plan and sequence the movements required for speech. This is why the framework quantifies variables such as jaw grading, lingual dissociation, and articulatory trajectory. However, the child’s goal in therapy is not simply to produce movements accurately—it is to communicate successfully and be understood.
If a target word is motorically easy (low TMS) but has little meaning or usefulness in the child’s daily life, mastering that word may have minimal impact on overall intelligibility or functional communication. In other words, accurate production alone does not guarantee meaningful communication.
7.2 The “Functional Override”
For children with severe CAS and significantly reduced intelligibility, the immediate clinical priority should be functional communication. This often requires targeting high-frequency, high-impact words (e.g., “stop,” “help,” “mine,” “go”), even when those words contain motorically complex features such as clusters, mid-vowels, or rapid transitions (high TMS scores).
* Early success in being understood—by caregivers, peers, and teachers—supports motivation, participation, and confidence, while also providing a meaningful and natural context for practicing motor planning skills.
7.3 Progressive Integration
Once a basic level of functional intelligibility is established, the Oral Motor Complexity Score becomes the primary framework for systematic expansion. Clinicians can then use the scoring system to intentionally scaffold motor difficulty, gradually introducing more complex vowels, syllable shapes, and articulatory transitions as the child’s motor planning abilities stabilize and improve
VIII. Conclusion
The Oral Motor Complexity Score v.2 provides a structured, biomechanically informed framework for designing and sequencing intervention targets in pediatric motor speech disorders (CAS). By integrating kinematic principles—such as jaw grading, movement trajectory cost, and inter-articulatory coordination—into target selection, clinicians can systematically manipulate motoric demands during therapy rather than merely describe performance. The TMS v.2 is intended to support intervention planning by allowing clinicians to calibrate task complexity, scaffold motor learning, and reduce unnecessary cognitive–linguistic load for children with complex motor speech deficits. In this way, the framework represents a step toward precision-based intervention in Speech-Language Pathology, rather than a diagnostic assessment tool.
Annex A: Master Library of Co-Articulation Compatibility
Use this reference guide to determine the correct Context Multiplier for specific target sounds.
1. The Lip Group (Labials) Biomechanical Focus: Lip Closure, Rounding, and Jaw Stability.
A. Labiodentals (/f/, /v/)
The Conflict: Lip Rounding. You cannot effectively "tuck" (labiodental contact) and "round" at the same time.
- Inhibitory (x 2.0): Round Vowels (/u/, /o/, /ɔ/).
- Facilitative (x 0.5): Spread/Neutral Vowels (/i/, /e/, /æ/).
B. Bilabials (/p/, /b/, /m/)
The Conflict: Jaw Tension.
- Neutral (x 1.0): Front/Spread Vowels (/i/, /e/, /æ/, /eɪ/). Lip closure does not mechanically assist or hinder lip spreading
- Facilitative (x 0.5): Central Vowels (/ə/, /ʌ/). Relaxed jaw aids closure.
- Resonance Rule (/m/): Inhibitory (x 2.0) when adjacent to an Oral Stop (e.g., "camp") due to rapid valving switch.
C. The Labio-Velar Glide (/w/)
The Conflict: Un-rounding.
- Facilitative (x 0.5): Round Vowels (/u/, /o/, /ɔ/). Lips are already in position.
- Inhibitory (x 2.0): Spread Vowels (/i/, /e/). Requires rapid movement from round to spread.
2. The Tongue Tip Group (Anterior) Biomechanical Focus: Moving the tongue tip forward.
A. Interdentals (/θ/, /ð/)
The Conflict: Tongue Retraction.
- Inhibitory (x 2.0): Back Vowels (/u/, /o/, /ɑ/).
- Facilitative (x 0.5): Front Vowels (/i/, /e/, /æ/).
B. Alveolars (/t/, /d/, /n/, /s/, /z/)
The Conflict: Tongue Backing.
- Inhibitory (x 2.0): Back Vowels (/u/, /o/, /ɑ/).
- Facilitative (x 0.5): Front Vowels (/i/, /e/).
- Resonance Rule (/n/): Inhibitory (x 2.0) when adjacent to an Oral Stop (e.g., ‘ant’, ‘hand’) due to rapid valving switch.
3. The Tongue Body Group (Posterior & Complex) Biomechanical Focus: Tongue height and shape.
A. Palatals & Affricates (/ʃ/, /ʒ/, /ʧ/, /ʤ/, /j/)
The Conflict: Low Jaw Position.
- Facilitative (x 0.5): High Vowels & Round Vowels (/i/, /u/). Maintains high jaw and rounding.
- Inhibitory (x 2.0): Low Vowels (/ɑ/, /æ/). Forces the jaw open, destabilizing the tongue.
B. Velars (/k/, /g/, /ŋ/)
The Conflict: Tongue Fronting.
- Inhibitory (x 2.0): High Front Vowels (/i/, /e/).
- Facilitative (x 0.5): Back Vowels (/u/, /o/, /ɑ/).
- Resonance Rule (/ŋ/): Inhibitory (x 2.0) in common clusters like /ŋk/ ("sink") due to resonance conflict.
4. The Liquid Group (Complex) Biomechanical Focus: Unique internal tension.
A. The Lateral (/l/)
- Pre-Vocalic (Light L): Facilitated by Front Vowels.
- Post-Vocalic (Dark L): Inhibitory (x 2.0) in almost all contexts.
B. The Rhotic (/r/)
The Conflict: Instability.
- Inhibitory (x 2.0): Round Vowels (unless rounded-R) and Low Vowels.
- Facilitative (x 0.5): Central Vowels (/ə/, /ʌ/, /ɝ/). The "neutral zone" provides stability.
5. The Glottal (/h/)
- The Rule: Adopts the posture of the subsequent vowel nucleus.
- Neutral (x 1.0): Because /h/ requires no independent lingual or labial positioning, it maintains a neutral kinematic relationship with all vowels.
Annex B: How to use this tool in therapy: "Building a Path to Success"
1. Longer words are not always harder
One of the most important things this tool shows is that a long word can actually be easier to say than a short word. Think of it like walking:
- Taking three easy steps on flat ground (Banana) is easier than taking two giant leaps over a wide hole (Table).
- Banana uses "baby sounds" like /b/ and /n/ and the mouth does the same easy movement over and over.
- Table is shorter, but the tongue has to do a very difficult "gymnastic" move for the /l/ sound at the end.
2. How to choose the right words
When you are working with a child, you should use the TMS Score as your guide, not the number of letters or syllables.
- Start with Low Scores:
Always start therapy with words that have the lowest scores (like 4.0 to 9.0). These are the "Easy Wins."
- What to do if a child struggles:
If a child is having a hard time with a word, don't just look for a shorter word. Look for a word with a lower score.
- The Goal:
We want the child to feel successful. By picking words with low scores, we make the "work" easier for their mouth. This helps them practice more without getting frustrated.
3. A Guide for Parents and Assistants
- The "Motor Plan" is like a Recipe:
Some recipes have many steps but are very easy (like making a sandwich).
Some recipes have only two steps but are very hard (like soufflé).
- Use the Tool to check the "Recipe":
Before you give a child a list of words to practice, run them through our script.
If a word has a high score (like 18 or 20), it might be too "heavy" for the child right now.
- Drop the Weight:
If the child is "tripping" over their words, go back to a word with a lower score to help them get their confidence back.
Why this tool is special (The "Bottom Line")
I created this tool because I wanted to stop "guessing" which words are hard. This tool gives us a number that tells us exactly how much effort the child's mouth has to use. If the score is low, the effort is low. That is where we start.
Use this reference guide to determine the correct Context Multiplier for specific target sounds.
Note on Co-Articulation, Vowels, and Categorical Interpretation
While the TMS v.3 incorporates well-established principles from articulatory phonetics and motor speech research, it is essential to clarify the nature and limits of the vowel–consonant co-articulation rules described in this framework.
The Context Multipliers presented in Annex A are not intended to represent categorical phonological constraints or universal articulatory prohibitions. In typically developing English speakers, all vowel–consonant combinations described in this framework are phonotactically legal and can be produced with high accuracy under normal conditions. The designations “facilitative” and “inhibitory” should therefore be interpreted relatively rather than absolutely.
Specifically:
- “Inhibitory” contexts do not imply that a vowel or consonant is intrinsically difficult or unachievable, but rather that the articulatory gestures involved may require greater gestural distance, tighter temporal coordination, or increased independence between articulators.
- “Facilitative” contexts do not eliminate motor demands, but may reduce the degree of adjustment required due to shared or compatible articulatory postures (e.g., lip rounding, tongue body position, or jaw height).
Importantly, co-articulation in English is gradient and adaptive, not conflict-based. Speakers routinely resolve competing articulatory demands through timing shifts, spatial undershoot, or gestural blending. The present framework models relative motor planning load, not mechanical interference or articulatory failure.
Furthermore, vowel categories used in this framework (e.g., “front,” “back,” “rounded,” “central”) represent functional groupings for clinical modeling, not claims about uniform articulatory behavior across all dialects, speaking rates, or individuals. The magnitude of co-articulatory effects varies based on:
- Speech rate and prosodic context
- Stress and syllable structure
- Developmental stage
- Individual motor control profiles, particularly in Childhood Apraxia of Speech
Finally, the vowel hierarchy and co-articulation multipliers proposed here are theoretically motivated but not yet empirically validated using direct kinematic measures (e.g., ultrasound tongue imaging, EMA, or real-time MRI). They should therefore be applied as clinical heuristics to guide scaffolding and target selection, rather than as fixed rules or diagnostic thresholds.
________________
* In this framework, the term kinematic refers to articulatory movement patterns (distance, velocity, and coordination) rather than acoustic or phonological properties.
Annex C: Technical Implementation & Clinical Workflow
How to Use the TMS v.3 Analysis Tool
Follow these steps to generate motor planning (TMS) scores for your child’s target words.
Step 1: Install Python (The Engine)
You only need to do this once
- Go to python.org and Download the latest version for your computer (Windows or Mac).
- IMPORTANT: When you start the installer, you must check the box that says "Add Python to PATH."
- Click Install Now and wait for the installation to finish.
Step 2: Install the Libraries (The Tools)
You only need to do this once.
- Open your Command Prompt (on Windows, type cmd in the search bar) or Terminal (on Mac).
- Type the following line exactly and press Enter:
- pip install python-docx eng-to-ipa
- Wait until the text finishes scrolling. When the prompt returns, the libraries are installed and ready.
Step 3: Prepare Your Folder and Files
Open File Explorer (Windows) or Finder (Mac).
- Create a new folder and name it SpeechTool
- Windows: place it at C:\SpeechTool | Mac: you may place it anywhere (Desktop is recommended).
- Download the specific analysis script you need from my website (slpa.ca)
- (e.g., b-TMS.py) and save it into the SpeechTool folder.
- Prepare your word list:
Open Microsoft Word and create a document named with the letter of the sound (e.g., B.docx)
- Type your target words separated by commas.
IMPORTANT: For words with more than one syllable, use a hyphen (-) to show the breaks based on "Clear Speech."
Divide the word based on how you say it, not how you spell it.
- Correct: ma-mmy (This matches the motor movement).
- Incorrect: mam-my (This is a spelling rule, not a speech rule).
- Example: ba-na-na, ba-by, ta-ble.
(Note: If you don't use a hyphen, the tool will try to guess the syllables, but for clear speech practice, it is best to provide them manually).
- Save this file in your SpeechTool At this point, your SpeechTool folder should contain:
- The Python script (e.g., b-TMS.py)
- The file docx
Step 4: Run the Analysis
- Open your Command Prompt or Terminal again (on Windows, type cmd in the search bar) or Terminal (on Mac).
- Type the following and press Enter:
- cd C:\SpeechTool (or drag the SpeechTool folder into the Terminal window and press Enter)
- Type this to run the script:
- python b-TMS.py (Note: If you downloaded a different sound, use that filename, like python p-TMS.py).
- Success! A new Word document named b-TMS-Results.docx will appear in your folder. Open it to see your scores.
Clinical Interpretation of Results
- Start with the Lowest Numbers: These are the "motoric easy wins."
- Trust the Kinematics: A 3-syllable word like ba-na-na may have a lower score than a 1-syllable word like brick because the motor transitions are simpler.
- Layer 2 Check: Look for "Basic Shape" vs "Complex Shape" (clusters). Master basic shapes first.
Download the specific analysis script you need
Technical Note on the Word Rankings
This list has been organized using a specialized computational system that ranks word difficulty based on the motor-planning movements required for clear speech. Because English phonetics are exceptionally complex, no digital analysis is 100% perfect.
You may occasionally find a word where the phonetic symbols or the difficulty score seem unusual—this is simply a technical limitation of the analysis system. If a specific word appears to be an error, please skip it and proceed to the next one. This list is intended as a helpful guide to prioritize practice, with over 95% of the data providing a reliable path for speech development.
- b-TMS.pyp-TMS.py
Download ready-made word lists
If you would like to see the word lists used for the scripts, they are provided here. Feel free to download and use them.
B.docxP.docxWord lists with Total Motor Scores (TMS) are also available through the Apraxia of Speech menu, organized by English consonant sounds, with each list showing the corresponding scores.
*** This page is still in progress. Scripts and documents will be added soon.
You are not authorised to post comments.
Comments will undergo moderation before they get published.